

{kind=link}
In early September, CHIR Assistant Analysis Professor Christine Monahan testified earlier than the Texas Home Insurance coverage Committee on outpatient facility price billing and potential reforms. The Texas legislature is at present getting ready for its 89th legislative session subsequent spring, and the current listening to will play a important function in shaping laws to return.
Christine’s feedback to the committee observe. A corresponding slide deck is obtainable right here.
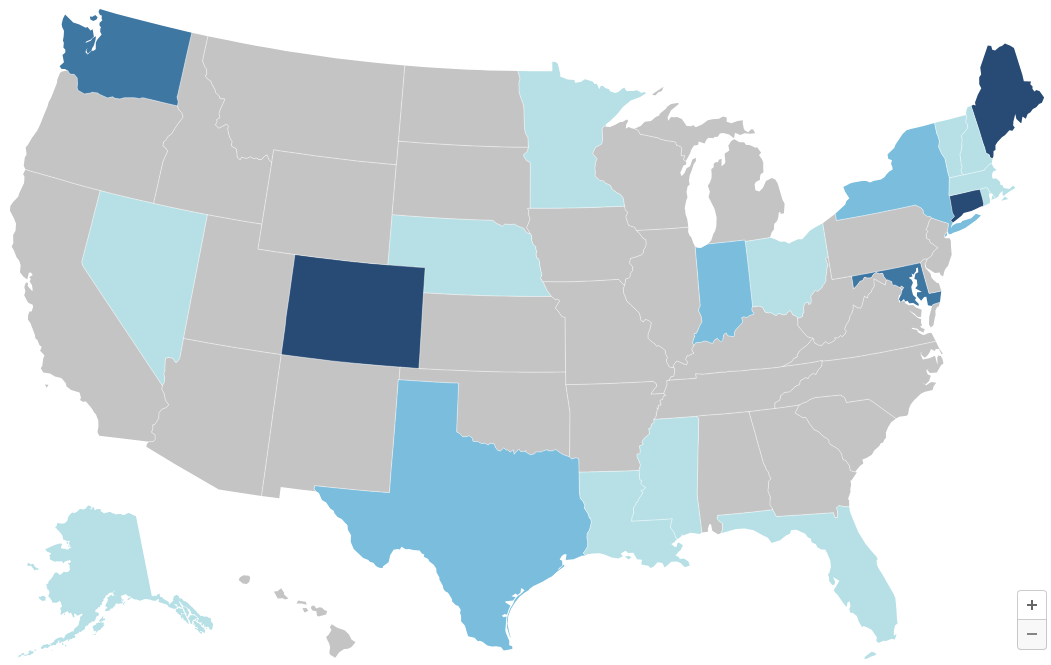
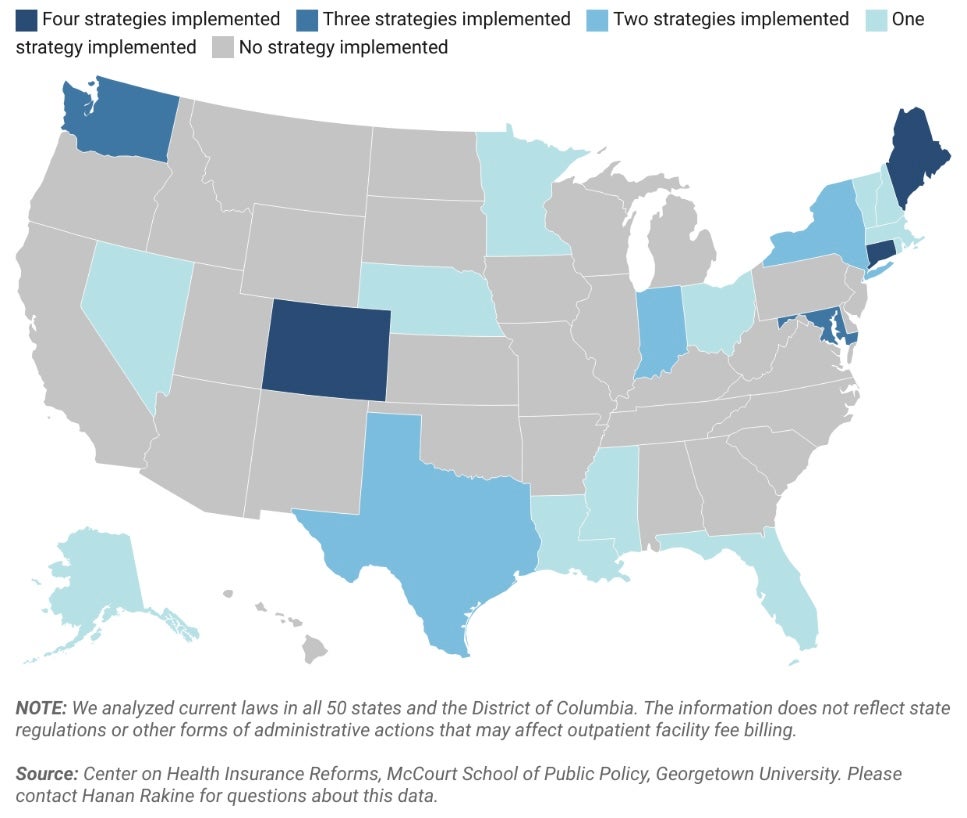
At CHIR, we research non-public medical insurance and well being care markets, conduct authorized and coverage evaluation, and supply technical help to federal and state policymakers, regulators and stakeholders on a spread of matters. With the assist of West Well being, I and several other members of the CHIR group have been finding out outpatient facility price billing for the previous two years. We have now carried out a number of dozen interviews with on the bottom stakeholders, reviewed current legal guidelines and pending laws at each the state and federal ranges, written a number of analyses, and, most just lately, revealed a collection of maps reporting on our overview of the legal guidelines in all 50 states and the District of Columbia associated to outpatient facility price billing.
Step one to understanding facility price billing is to grasp that there are two forms of claims usually used to invoice for medical providers: an expert invoice (the CMS-1500) and the ability invoice (the UB-04). In case you obtain care at an unbiased supplier observe, the supplier who handled you’ll submit an expert invoice to your insurer. This invoice, in idea, covers their time and labor in addition to any observe overhead prices, like nursing employees, lease, and gear and provides. However, for those who obtain care at a hospital outpatient division, typically talking any skilled who handled you, in addition to the hospital, will every submit separate payments. Any skilled payments ought to simply cowl the supplier’s time and labor, whereas the hospital invoice – or facility price – ostensibly covers overhead prices.
What counts as hospital overhead and what else goes right into a facility price is difficult, nevertheless. As you’ll count on, a facility price typically will cowl the overhead prices associated to the affected person go to for which it’s being billed, together with the nurses or assist employees concerned and any gear and provides. As a result of hospital outpatient departments want to fulfill further licensure and regulatory necessities, they seemingly even have some further prices that don’t apply to unbiased settings.
As well as, a facility price is prone to cowl different hospital overhead prices. A few of these are mandatory and fascinating providers on the inhabitants degree, however not associated to the care delivered to the affected person who’s getting billed. For instance, facility charges may assist fund issues like hospital emergency providers, or 24/7 staffing and safety on the hospital, despite the fact that the affected person was on the facility throughout regular enterprise hours and didn’t want any emergency care or they went to a very separate, off-campus facility ten miles from the hospital campus and emergency room. Hospital overhead prices can even embody issues of extra debatable worth – from excessive CEO salaries, to costly paintings or connoisseur meals providers, to, I child you not, film manufacturing studios. All of these items could also be thought of hospital “prices” that sufferers might be requested to pay via a facility price.
Additionally it is essential to know that different elements, unrelated to the price of care or different bills a hospital has, additionally play an enormous function in figuring out how a lot a hospital payments for and will get paid by insurers, together with historic billing patterns and market energy. Significantly as hospitals and well being techniques get greater, and vertically combine, they’ve rather more energy than your solo doctor or unbiased group observe to demand larger reimbursement when negotiating with insurers.
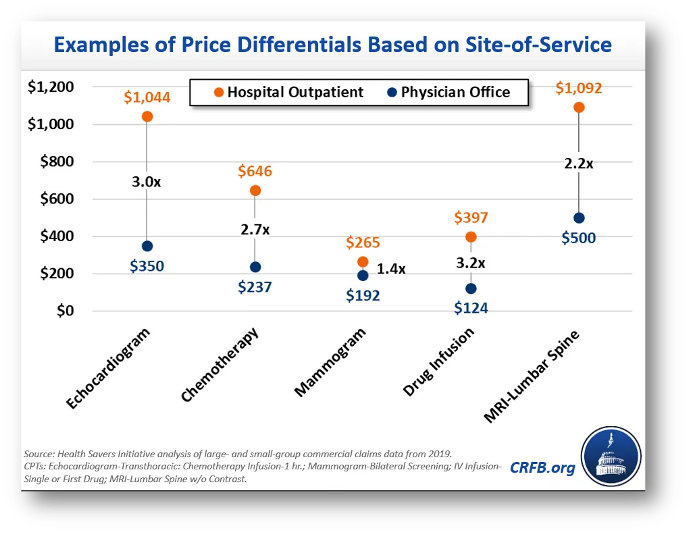
So, when financial specialists evaluate the costs paid for a similar providers at hospital outpatient departments and unbiased doctor places of work, they discover a lot larger costs in hospital settings. Chemotherapy is one instance from the Committee for a Accountable Federal Funds. A affected person going for weekly chemotherapy visits would see, on common, a 2.7-fold distinction in worth in the event that they switched from an unbiased observe to a hospital outpatient division. And, in fact, they’re typically not those making that selection to modify – moderately, sooner or later in the course of remedy they could go into the identical workplace constructing as at all times, for a similar care as at all times, and are available away with a invoice that’s greater than $400 larger than what they’re used to as a result of a hospital acquired their observe and transformed it to a hospital outpatient division.
It’s this current historical past of aggressive hospital acquisition of outpatient practices that’s driving the problem in the present day. Facility price billing just isn’t a novel observe, however it’s extra widespread than it was once following years of vertical integration the place hospitals are buying or constructing their very own outpatient doctor practices and clinics. Certainly, one of many causes hospitals and well being techniques have considerably expanded their possession and management over outpatient doctor practices over the previous decade or so, is so they may cost this second invoice and improve their revenues.
One other seemingly purpose we’re listening to about facility price billing extra now are inadequacies in insurance coverage protection. Because the hospital business will emphasize, sufferers more and more are coming in with excessive deductible well being plans which depart them uncovered to extra expenses, together with facility charges. The hospitals will not be improper in stating this hole, however it’s best understood as a symptom of the better drawback of rising costs.
Increased spending on outpatient care from facility price expenses is rising the price of medical insurance for all of us: sufferers and shoppers who enroll in medical insurance, employers who’re sponsoring insurance coverage for his or her employees and paying greater than 70-80% of their well being plan premiums, and taxpayers who closely subsidize the non-public medical insurance market. Economist Stephen Parente, who served on the White Home Council of Financial Advisers within the Trump Administration, just lately launched a research discovering that employer plan premiums may go down greater than 5% yearly if insurers paid the identical quantity for care in a hospital outpatient division as they do an unbiased doctor’s workplace. This in flip would end in $140 billion in financial savings to the federal authorities over ten years via decreased tax subsidies for employer plans. Whereas not the one issue, outpatient facility price billing is contributing to the rising unaffordability of medical insurance in the present day.
On the similar time, insurers are responding to those worth will increase largely by rising cost-sharing and in any other case limiting advantages. Because the hospital business factors out, medical insurance deductibles are rising in measurement and prevalence. A lot of these $200, $300, $400+ facility charges are going straight to the affected person. Customers can also face larger cost-sharing for care supplied at a hospital outpatient division even when their deductible doesn’t apply. This may be as a result of the ability price is carrying its personal distinct cost-sharing obligation from the skilled invoice or as a result of insurers set larger cost-sharing charges for providers supplied at hospital outpatient departments to attempt to discourage sufferers from going to them. Moreover, some insurers could merely not cowl a service when it’s supplied at a hospital outpatient division, in an effort to comprise their very own spending whereas doubtlessly opening up sufferers to steadiness billing.
In sum, inadequacies in insurance coverage protection are enjoying a job in exposing shoppers to excessive medical payments which is driving media consideration. But when insurance coverage coated these expenses with none cost-sharing, shoppers in addition to employers and taxpayers would nonetheless be paying for it via their premium {dollars} – it simply can be much less seen.
What, then, might be accomplished to deal with these considerations? One possibility is to proceed to attend to see if the non-public market will repair it. However there are obstacles to personal reforms, together with a ignorance, a scarcity of leverage, and a scarcity of motivation.
With respect to info, one of many refrains we constantly hear from stakeholders is that there are important gaps in claims information that make it difficult for personal payers and regulators alike to grasp the total scope and impression of facility price billing. Particularly, they reported that it may be very tough if not inconceivable to determine the precise brick and mortar location the place care was supplied on a claims type or in a claims database. The tackle line may consult with the primary campus of a hospital that owns the observe, and even an out-of-state billing workplace for the well being system.
By way of leverage, dominant hospitals often have the upper-hand in negotiations with insurance coverage corporations as a key promoting level for insurers is that they’ve the identify model hospital or doctor group of their community. In Massachusetts, one of many main insurers proactively sought to get rid of outpatient facility price billing by in-network suppliers, however may solely do that in a price range impartial method (agreeing to boost charges elsewhere to make up the distinction) and nonetheless one main well being system has refused to play ball and continues to invoice facility charges in the present day. Reforms like prohibiting anticompetitive contracting clauses, as Texas has enacted, could start to chip away at elements contributing to hospitals’ dominance in negotiations nevertheless.
Concerning motivation, insurers typically don’t profit from decreasing well being care prices as they take house a proportion of spending. However public scrutiny on egregious facility charges in Massachusetts motivated the insurer I beforehand talked about to behave, and will encourage different insurers elsewhere to observe swimsuit. Moreover, giant employers more and more are participating on this and different well being care spending points, and they are able to stress insurers to get rid of facility price billing of their contracts with suppliers. Certainly, I do know of not less than two state worker well being plans which have accomplished so.
In the end, although, facility price billing and different aggressive hospital pricing and billing practices are an uphill battle for the non-public market to deal with alone. Accordingly, we’re seeing states throughout the nation, reflecting broad geographic and political range, start to pursue legislative reforms. By our rely, twenty states nationwide have enacted a number of of the six potential options our group has recognized: website impartial fee reforms, facility price billing bans, billing transparency necessities, public reporting necessities, cost-sharing protections, and shopper notification necessities. I’m going to deal with simply the primary three I discussed proper now, however we’ve got further info on others and I’m blissful to debate any of them. Importantly, none of those reforms are mutually unique. They merely deal with the problems from completely different, however complementary angles.
First, states are starting to deal with the transparency points I simply raised. Notably Colorado, Nebraska, and Nevada now require off-campus hospital outpatient departments to amass a novel, location-specific supplier identifier quantity – often known as an NPI – and embody it on claims varieties. This can be a easy and minimally burdensome reform that will significantly improve claims information. As Colorado has realized, pairing this information with a system for monitoring which NPI belongs to which well being system could make it much more helpful, as it could give visibility into each the situation of care and who owns that setting. This info may assist non-public payers or regulators and policymakers rein in outpatient facility price billing. It additionally might be useful in serving to payers undertake tiered supplier networks or in any other case steer sufferers in direction of or away from completely different supplier places based mostly on the standard or price of care they supply.
A state looking for to go additional than that might prohibit hospital outpatient departments from charging facility charges for specified providers. Texas, in fact, has already accomplished this very narrowly for providers like Covid-19 exams and vaccinations when carried out at drive-through clinics at free-standing emergency departments. States like Connecticut, Maine, and Indiana, nevertheless, have extra broadly prohibited hospitals and well being techniques from charging facility charges for outpatient analysis and administration providers or different office-based care in sure settings.
By prohibiting facility charges for specified providers, policymakers defend sufferers from doubtlessly bearing the cost-sharing brunt of two payments. For instance, moderately than owing a $30 copay on the doctor’s invoice and a 40% coinsurance cost on the ability price, the affected person will return to owing only a $30 copay, as if they’d acquired care in an unbiased setting. For the big proportion of the inhabitants who wouldn’t have sufficient money to pay typical non-public plan cost-sharing quantities, this can be a actually massive deal. On the similar time, the system-wide financial savings from such a reform seemingly can be comparatively muted in the long term, as market highly effective hospitals renegotiate their contracts and improve different costs to make up for the lack of income from facility charges, as we noticed occur in Massachusetts.
Lastly, policymakers who’re feeling notably formidable could wish to contemplate site-neutral fee reforms, which is what Stephen Parente was finding out. These reforms name for insurers to pay the identical quantity for a similar service, no matter whether or not the service was supplied at a hospital outpatient division or an unbiased observe.
How this works, and the way massive of an impact it could have, rely on quite a lot of design selections. As with facility price bans, one of many important decisions can be what providers are coated and this might be broad or slender. Simply as essential is who determines how a lot insurers pay for a service and the way this fee degree compares to current costs. Below essentially the most hands-off model of a site-neutral coverage, lawmakers may merely require that insurers undertake site-neutral funds with out specifying a fee degree and leaving that to personal market negotiations. Alternatively, lawmakers may determine, or job regulators with figuring out, a benchmark degree be it tied to current industrial charges or a public price schedule, similar to a proportion of Medicare. The extra providers coated and the decrease the fee degree, the better the financial savings.
No state at this level has enacted a site-neutral coverage within the industrial sector up to now, however there’s rising curiosity and I anticipate that we are going to see some site-neutral payments launched within the coming yr.
Thanks for having me.